Acromioclavicular Dislocation

A common rugby and football injury.
Disruption of the ligaments by which the clavicle helps to suspend the scapula results in increased prominence of the clavicle. The function of the shoulder is not usually seriously impaired once the discomfort of the acute injury subsides.
INCIDENCE
- Varies with activity levels
- Common in athletes participating in football, wrestling, and lacrosse
- Most common in the 16- to 30-year age group
- Rare in skeletally immature individuals
- More common in males because of sports preferences
The Rockwood classification (1998) is the most common classification system in use for acromioclavicular joint injuries This well known 6-type system is a modification of the earlier 3-class classification system described by Allman (1967) 2 and Tossy (1963).
It takes into account not only the acromioclavicular joint itself but also the coracoclavicular ligament, the deltoid and trapezius muscles, and the direction of dislocation of the clavicle with respect to the acromion. Essentially types IV, V, and VI are variants of type III .
- type I: clavicle not elevated with respect to the acromion
- AC ligament: mild sprain
- CC ligament: intact
- joint capsule: intact
- deltoid muscle: intact
- trapezius muscle: intact
- type II: clavicle elevated but not above the superior border of the acromion
- AC ligament: ruptured
- CC ligament: sprain
- joint capsule: ruptured
- deltoid muscle: minimally detached
- trapezius muscle: minimally detached
- type III: clavicle elevated above the superior border of the acromion but coracoclavicular distance is less than twice normal (i.e. < 25 mm)
- AC ligament: ruptured
- CC ligament: ruptured
- joint capsule: ruptured
- deltoid muscle: detached
- trapezius muscle: detached
- type IV: clavicle displaced posterior into trapezius
- AC ligament: ruptured
- CC ligament: ruptured
- joint capsule: ruptured
- deltoid muscle: detached
- trapezius muscle: detached
- type V: clavicle is markedly elevated and coracoclavicular distance is more than double normal (i.e. > 25 mm)
- AC ligament: ruptured
- CC ligament: ruptured
- joint capsule: ruptured
- deltoid muscle: detached
- trapezius muscle: detached
- type VI: clavicle inferiorly displaced behind coracobrachialis and biceps tendons, which is rare
- AC ligament: ruptured
- CC ligament: ruptured
- joint capsule: ruptured
- deltoid muscle: detached
- trapezius muscle: detached
CAUSES
A fall or blow on the very tip of the shoulder (acromion) causes the scapula to be pushed down from the clavicle and damages the suspensory ligaments.
RISK FACTORS
- Contact sports
- Fall on point of elbow, with fall not broken by arm
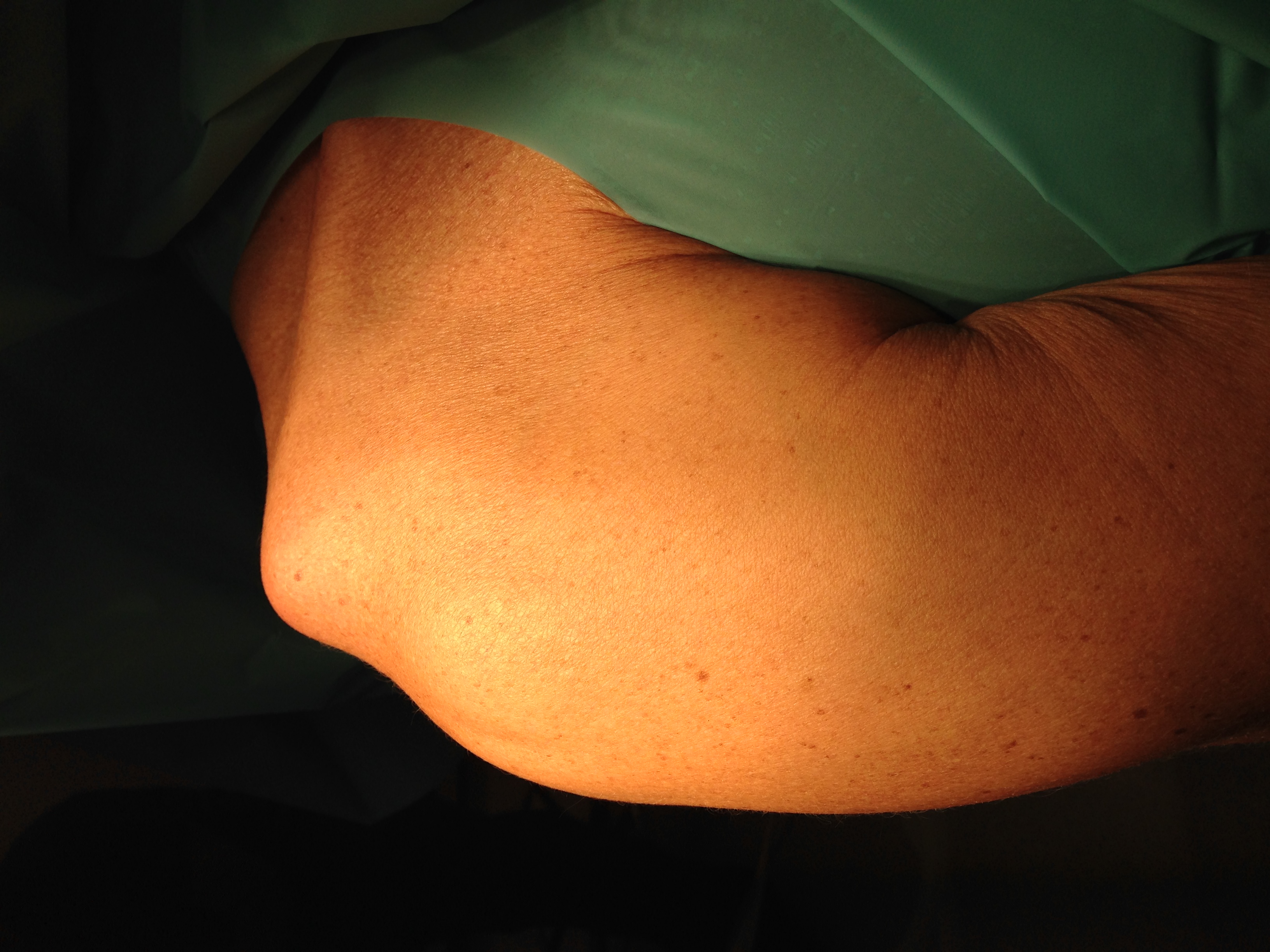
SIGNS AND SYMPTOMS
- Prominence on the "point" of the shoulder (clavicle)
- Scapula appearing to sag temporarily
- Tenderness in the area of lateral clavicle
- Shoulder movement in all directions painful
- Symptoms usually subsiding over 4 to 8 weeks and rarely recurrent
- A persistent ache with activity in a few patients
DIFFERENTIAL DIAGNOSIS
This includes clavicle fracture, in which tenderness is usually located more medially, and there is more swelling. A variant of this problem is the epiphyseal separation of the clavicle.
PHYSICAL EXAMINATION
Palpate for tenderness over the coracoclavicular ligaments and the acromioclavicular areas. Palpate the rest of the clavicle and the humerus for fracture. Ask the patient to actively abduct the shoulder and look for at least some muscle contraction in the rotator cuff.
PATHOLOGIC FINDINGS
Disruption in the acromioclavicular ligaments and coracoclavicular ligaments is seen, depending on the grade of injury.
IMAGING PROCEDURES
An anteroposterior radiograph of both shoulders allows comparison between the injured and uninjured sides. The distance between the coracoid and the clavicle may be compared. In grade I and II injury, the two sides are equal, but by adding weights to the hand, the distance may increase in grade II. In grade III, the distance is increased even without weights.
GENERAL MEASURES
Nonsteroidal antiinflammatory drugs or narcotic analgesics are given for the acute injury. A sling should be worn when the patient is up. Braces to reduce the joint (i.e., Kenny-Howard brace) are no longer widely used because of the risk of pressure sores and because of good results with only a simple sling. For patients with grade IV injuries, surgery may be indicated.
Gentle range of motion, then active use of the shoulder may be allowed as symptoms permit. Return to sports should be delayed at least for 6 weeks for patients with grades II to IV injuries.
SURGICAL TREATMENT
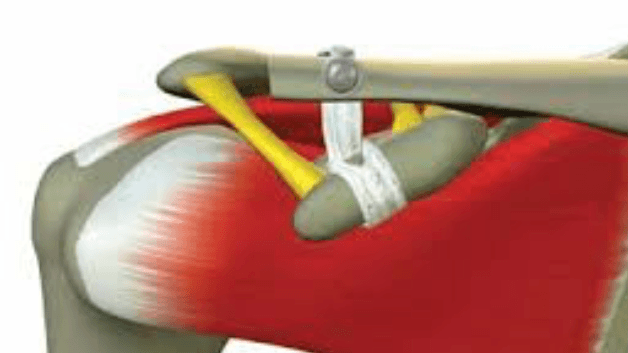
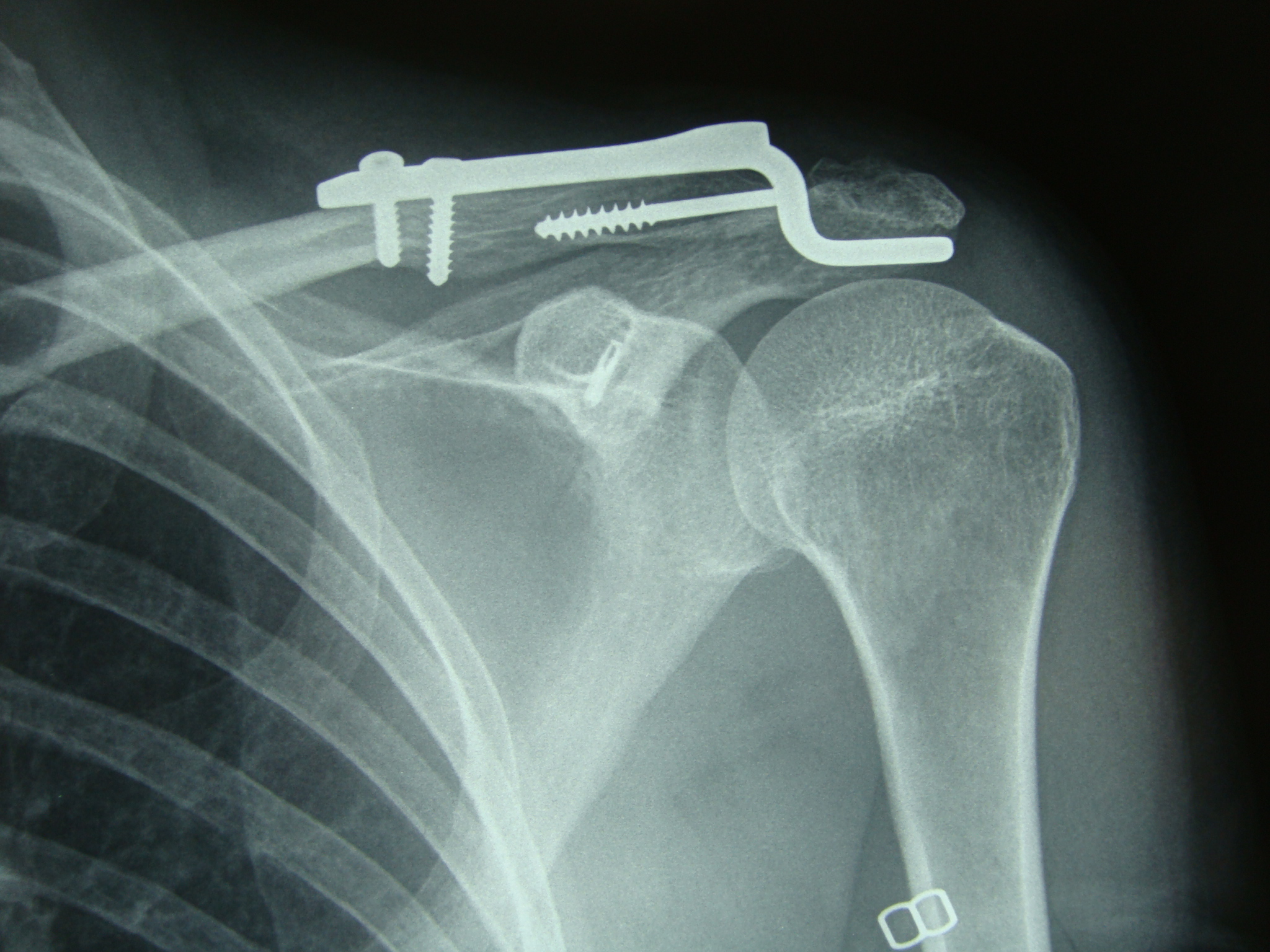
If surgery is indicated, the joint may be held in reduction with a screw or with ligament reconstruction.We use lockdown Surgilig ligament in some severe cases we use the hook plate as a secondary fixation.
The surgery is day case and use of polysling with ice pack is commenced afterwords. The scar is bra strap.
PHYSICAL THERAPY
This is indicated in severe cases. The therapist should work first on motion, then on strength. Home exercises should also be taught.
MEDICAL TREATMENT
An analgesic of choice is given for 2 to 4 weeks.
MONITORING
Focus on the patient's function. The radiographic appearance of the joint does not correlate with function, so routine follow-up radiographs are not typically needed.
COMPLICATIONS
Mild pain may persist, exacerbated by activity. In rare cases, painful arthrosis may occur.
PROGNOSIS
Most patients may return to their usual activities in several months. A few require reconstructive surgery, owing to persistent pain in the acromioclavicular joint.
- Lockdown ligament Below
- Modified Weaver-Dunn with hook plate
- All arthroscopic Tightrope procedure we have large experience with all of the above and more.