
Subacromial Impingement
Description
Impingement syndrome and subacromial bursitis are inflammations of the shoulder subacromial bursa and rotator cuff tendons (supraspinatus, infraspinatus, teres minor, and subscapularis muscles). The inflammation is often due to their impingement between the humeral greater tuberosity and the lateral structures of the shoulder (acromion, coracoacromial ligament, coracoid process, and acromioclavicular ligament). The impingement causes a continuum from chronic bursitis to complete rotator cuff tears. Patients of any age can be affected. However, there is a significant increasing incidence with age, as shown later in the section on classification. An accumulation of wear and impingement over the years leads to an increased incidence with increasing age.
Synonyms
- Subacromial bursitis
- Subacromial impingement
- Rotator cuff tendinitis
Incidence
These conditions are common, especially in older age groups and in athletes performing overhead activities (e.g., swimming, tennis).
Causes
Impingement of the rotator cuff tendons and subacromial bursa between the humeral head, greater tuberosity and the lateral structures of the shoulder (acromion, coracoacromial ligament, coracoid process, and acromioclavicular ligament) occurs when the arm is elevated. This causes inflammation and edema and therefore increased impingement, in a self-perpetuating cycle.
- Acromial shape: A hooked lateral surface (as opposed to flat) may increase impingement.
- Posterior shoulder capsule stiffness may force the humeral head upward, thereby increasing impingement.
- Rotator cuff weakness or tear causes a decrease in the humeral head depressor mechanism, thus increasing impingement.
Risk Factors
- Middle and older age (40 to 85 years)
- Increased overhead activities (e.g., lifting, swimming, tennis)
- Acromial shape: hooked lateral surface (as opposed to flat) possibly increasing impingement
Classification
Stage I: Patients Less than 25 Years Old Reversible edema and hemorrhage
Stage II: Patients 25 to 40 Years Old Fibrosis and tendinitis Pain recurring with activity
Stage III: Patients More than 45 Years Old Bone spurs and rotator cuff tendon rupture
Association Conditions
- Rotator cuff tears (95% of cuff tears associated with impingement)
- Calcific tendinitis
- Biceps tendinitis
- Acromioclavicular arthritis
- Frozen shoulder Diagnosis
Signs And Symptoms
- Inability to use the arm in the overhead position (flexed and internally rotated) because of pain, stiffness, weakness, and catching
- Pain with sleeping on the affected side
- Pain in the acromial area
Differential Diagnosis
Many of these conditions are associated with impingement:
Cuff tears
- Symptoms
- Shoulder pain
- Inability to lift the arm
- Pain with motion
- Identified with magnetic resonance imaging
- Ninety-five percent of cuff tears associated with impingement Calcific Tendinitis
- Localized tenderness
- Possibly associated with impingement from increased size of the tendon
- Diagnosed with radiographs Biceps Tendinitis
- Pain to palpation in the biceps groove Cervical Radiculopathy
- Pain on turning the head Radiculopathy
- Diagnosed with electromyography Acromioclavicular Arthritis
- Acromioclavicular joint tenderness to palpation
- Radiographs showing degenerative changes in the joint
- Diagnosed with injection of lidocaine into the acromioclavicular joint Glenohumeral Instability
- Diagnosed with physical examination Degeneration of the Glenohumeral Joint
- Diagnosed with radiographs Stiff or Frozen Shoulder
- Diagnosed with physical examination
- Restricted range of motion with passive range of motion equal to active range of motion
Physical Examination
- Atrophy of rotator cuff muscles
- Decreased range of motion, especially internal rotation and cross body adduction, from posterior capsular tightness
- Weakness in flexion and external rotation
- Pain on resisted abduction and external rotation
- Pain on "impingement signs"
- Neer's impingement sign: passive elevation of the arm in the sagittal plane (shoulder flexion)
- Hawkins' impingement sign: with the elbow flexed to 90 degrees, the shoulder passively flexed to 90 degrees and internally rotated
Laboratory Tests
- Subacromial injection-impingement test:
- Inject 10 mL of 1% lidocaine into the subacromial bursa. If there is a significant reduction in the patient's pain, this is a positive impingement test.
Pathological Findings
Degeneration of the supraspinatus tendon
Imaging Procedures
- Plain Radiography Anteroposterior
- Subacromial sclerosis ("eyebrow sign")
- Greater tuberosity cyst
- Superior migration of the humeral head Thirty-Degree
- Caudad Angled Anteroposterior View
- Subacromial proliferation Lateral Scapular Supraspinatus Outlet View
- Showing type of acromion (flat, rounded, or hooked) Magnetic Resonance Imaging
- Used to diagnose a rotator cuff tear Diagnosis
Differential Diagnosis
Many of these conditions are associated with impingement:
Cuff tears
- Symptoms
- Shoulder pain
- Inability to lift the arm
- Pain with motion
- Identified with magnetic resonance imaging
- Ninety-five percent of cuff tears associated with impingement Calcific Tendinitis
- Localized tenderness
- Possibly associated with impingement from increased size of the tendon
- Diagnosed with radiographs Biceps Tendinitis
- Pain to palpation in the biceps groove Cervical Radiculopathy
- Pain on turning the head Radiculopathy
- Diagnosed with electromyography Acromioclavicular Arthritis
- Acromioclavicular joint tenderness to palpation
- Radiographs showing degenerative changes in the joint
- Diagnosed with injection of lidocaine into the acromioclavicular joint Glenohumeral Instability
- Diagnosed with physical examination Degeneration of the Glenohumeral Joint
- Diagnosed with radiographs Stiff or Frozen Shoulder
- Diagnosed with physical examination
- Restricted range of motion with passive range of motion equal to active range of motion
Physical Examination
- Atrophy of rotator cuff muscles
- Decreased range of motion, especially internal rotation and cross body adduction, from posterior capsular tightness
- Weakness in flexion and external rotation
- Pain on resisted abduction and external rotation
- Pain on "impingement signs"
- Neer's impingement sign: passive elevation of the arm in the sagittal plane (shoulder flexion)
- Hawkins' impingement sign: with the elbow flexed to 90 degrees, the shoulder passively flexed to 90 degrees and internally rotated
Surgical Treatment
- Acromioplasty Indications No improvement after 6 months of conservative therapy Relief of pain with injection Postoperative Care
- Early range of motion critical to avoid adhesions
- Success rate typically 70% to 90% Reasons for Failure
- Inadequate or excessive resection of acromion
- Failure of deltoid reattachment
- Incorrect or incomplete diagnosis, such as acromioclavicular arthritis and impingement syndrome
- Postoperative adhesions Procedure:
An incision is made through the skin. The deltoid is then partially incised and is partially elevated off the acromion. The subacromial bursa is then removed. A 2.0 by 0.9 cm wedge is then taken from the anterior undersurface of the acromion including the coracoacromial ligament. The bone is smoothed. The deltoid is repaired to the acromion. The skin is closed. In some cases, this can be done with the arthroscope.Resect the acromioclavicular joint in the following situations:
- Severe arthritis
- Exposure to the supraspinatus needed
- Impingement felt during the operation
- Repair of torn rotator cuff
Physical Therapy
- Stretching and Range-of-Motion Exercises
- Relieve posterior capsule tightness
- Avoid frozen shoulder Strengthening Exercises
- Especially use internal and external rotator exercises
- Strengthen humeral head depressors
- Avoid exercises above the level of the shoulder that could cause impingement
Medical Treatment
- Initial nonoperative treatment includes the following: Modalities (No Optimal Protocol but Many Available)
- Rest
- Avoidance of painful and overhead activities that cause impingement
- Modification of work or sport that exacerbates symptoms
- Gradual conditioning before a return to activities Stretching and Range-of-Motion Exercises
- Relieve posterior capsule tightness
- Avoid frozen shoulder Strengthening Exercises
- Use internal and external rotator exercises, in particular
- Strengthen humeral head depressors
- Avoid exercises above the level of the shoulder that could cause impingement Other Measures
- Nonsteroidal antiinflammatory drugs and analgesics
- Ice (20 minutes twice daily), heat, massage
- Corticosteroid injections
- The success rate for these treatments is almost 90%.
Patient Education
Patients should understand the impingement syndrome and the need for rest, physical therapy, gradual conditioning before resuming regular activities, and other conservative measures to relieve the symptoms. They should also understand the continuum from chronic bursitis to a rotator cuff tear.
Prevention
Avoid overhead and painful activities.
Complications
- Rotator cuff tear
- Frozen shoulder
- Biceps tendon tear
Prognosis
- The success rate with conservative therapy is approximately 90%.
- Of those in whom conservative therapy fails, the surgical success rate is approximately 70% to 90%.
The painful shoulder: shoulder impingement syndrome.
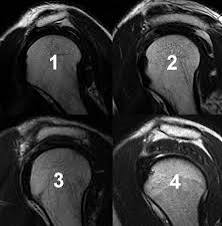
Acromion morphology (types) are based on sagittal oblique MRI:
- flat inferiorly (12%) 6
- curved (56%) parallel to the humeral head with a concave undersurface. ...
- hooked (29%) the most anterior portion of the acromion has a hooked shape. ...
- convex (upturned) (3%) most recent classification of acromion process shape.